Lennox-Gastaut Syndrome
LENNOX-GASTAUT SYNDROME
Introduction
Lennox-Gastaut (LGS) is an uncommon pediatric epilepsy syndrome that makes up around 10% of childhood epilepsy. Lennox-Gastaut is characterized by the onset of multiple different seizure types, severe cognitive delay, and a distinct EEG pattern.
History
Lennox-Gastaut is named after the two physicians who first documented the disease. In the 1950’s, Dr. William Lennox described a particular EEG finding that would match an epilepsy syndrome that Dr. Henri Gastaut was studying in the mid 1960’s. Dr. Henri Gastaut described a childhood epilepsy with frequent tonic and absence seizures. Later it was found that both Dr. Lennox and Dr. Gastaut were studying the same epilepsy syndrome and thus it was coined Lennox-Gastaut syndrome.
Symptoms
Lennox-Gastaut is frequently associated with intractable epilepsy, severe cognitive impairment, and characteristic EEG.
Epilepsy
Patients with Lennox-Gastaut tend to present with multiple seizure types.
- Tonic
- Tonic-Clonic
- Atonic (Drop attacks)
- Myoclonic
- Atypical Absence (With characteristic EEG pattern)
Seizures in patients with Lennox-Gastaut are frequent in nature and tend to cluster making them at high risk for evolving into Non-convulsive status epilepticus (NCSE) with some studies showing an incidence of NCSE being over.
The average of seizure onset in patients with LGS is between 3-5 years of age. Almost all patients with an LGS diagnosis have an onset of seizures before 8 years of age.
Cognitive Impairment
Cognitive impairment before seizure onset is seen in roughly half of patients. Depending on the severity of the disease there may be a delayed onset of cognitive delay after the patient has their first seizure.
Characteristic EEG pattern
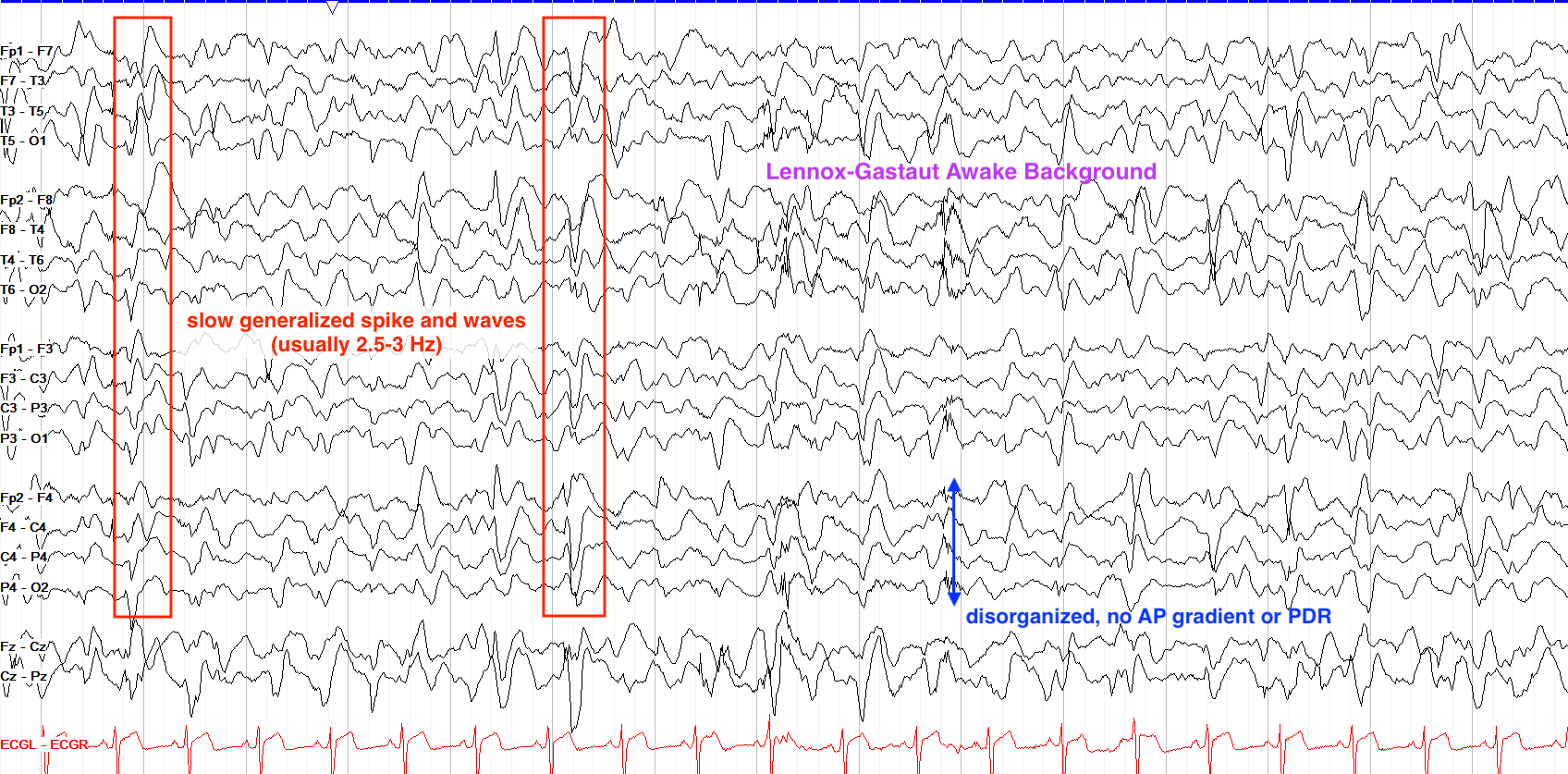
EEG in patients with LGS can be complex and difficult to read. Due to the multitude of seizure types, LGS seizure can present in several different ways which may make it difficult to differentiate the disease from others. However, in LGS there is a very characteristic EEG pattern known as atypical absence which helps to set it apart from others.
Atypical absence seizures are defined as slow (1.5-2.5 Hz) irregular polyspike and wave activity. It is important to note that atypical absence seizures differ from typical absence seizures in that they are slower (Typical absence seizures tend to be in the 3-5 Hz range) and are often asymmetric (Typical absence seizures are almost always generalized). Atypical absence seizures are NOT triggered by hyperventilation.
From “The Pediatric EEG”, by David Valentine M.D., 2020, (https://www.learningeeg.com/pediatric). Copyright 2020 by David Valentine
Figure 2.1 showing Lennox Gastaut awake background with 2-2.5 Hz generalized spike and wave.
Other patterns that can be seen in Ictal EEG of an LGS patient include:
- Rhythmic, high amplitude discharges in the high alpha-beta ranges seen in tonic seizures.
- Arrhythmic bursts of polyspike-wave discharges seen in myoclonic seizures.
Classifications of disease
LGS diagnoses typically fall into the following two categories: Secondary & Idiopathic
Secondary LGS:
This accounts for about 75% of all cases and describes a known primary cause. Any damage to the brain before or during birth can be considered a primary cause to LGS. These include:
- Infection
- Frontal lobe injury
- Tuberous Sclerosis
- Perinatal asphyxia
- Perinatal stroke
- Abnormal development
Idiopathic LGS
These account for the other 25% of LGS cases and have no known cause.
Linkage between Lennox-Gastaut & West Syndrome
An LGS diagnosis has been to known to frequently follow a myriad of other childhood epilepsy diagnoses. None are more common than the diagnosis of West Syndrome, as many LGS cases follow a diagnosis of West Syndrome despite no known cause for the linkage of the two.
Treatments & Prognosis
Long-term prognosis is generally unfavorable for patients with LGS. While mortality secondary to LGS is low, severe cognitive impairment and treatment resistant epilepsy still persists in the majority of patients. Patients with a history of West Syndrome also tend to have worse outcomes than those with idiopathic LGS.
Treatment options in LGS vary due to the multitude of seizure types. Antiepileptic drugs (AEDs) tend to be the mainline treatment for LGS but rarely does a single AED give complete relief of seizures. Valproic Acid (Depakote) and Lamotrigine (Lamictal) are the most commonly used AEDs in LGS. Other forms of treatment include the Ketogenic Diet, VNS, and surgical intervention. LGS patients are good candidates for corpus callostomy to help reduce the frequency of seizures, though it is rare for surgical intervention to be completely curative.
Key Takeaways
- 1.5-2.5 Hz Absence seizures are a common EEG finding in patients with LGS.
- LGS is likely to be secondary to some form of neurological damage before or during birth.
- There is a common progression of West Syndrome to Lennox-Gastaut.
- Valproic acid is the mainline treatment for LGS, followed by a variety of other AEDs as needed.
Media Attributions
- U11-062c-Temporal-Lobe
Objective 1: Describe the evidence that prehistoric and indigenous humans were aware of brain function.
History of Neuroscience Objective 1 Video Lecture
Neuroscience is a field that is both ineffably ancient and incredibly modern. Humans have been curious about what makes the brains work for as long as we have been human; understanding that one has a brain and trying to understand how that brain interacts with the environment is the very essence of what neuroscience and psychology define as consciousness.
Yet, as new technologies beget new tools, our understanding of the brain becomes more and more precise. Ultimately, however, as we press our knowledge to the molecular level, we find that the billions of proteins which are unique to 80 billion brain cells each connected to 10,000 other brain cells begins to challenge the limits of our understanding.
Neuroscience as a field is incredibly young amongst the sciences. The word "neuroscience" was coined in 1962 by Francis O. Schmitt. Nine years later, the first Society for Neuroscience meeting was held in Washington, DC and attracted 1,200 people. Currently, the Society for Neuroscience meetings are so large that they can only be held in three US cities: Washington, Chicago, and San Diego, and each one attracts over 30,000 attendees. In a very literal sense, neuroscientists gathered together form a small city. Neuroscience contains all the elements of the acronym STEM: science, technology, engineering, and mathematics. Neuroscience has been, and will continue to be, informed by approaches from classical and quantum physics; from organic and physical chemistry; from ecology, cell biology, and molecular biology; and from the "top-down" scientific approaches of psychology.
Alison Gopnik, Andrew Melzoff, and Patricia Kuhl's book The Scientist in the Crib reminds us that we are all born scientists. Think about the challenge for a newborn baby. It is absolutely essential for the survival of the species that a newborn human eagerly pursues two imperatives: food and shelter. Yet, armed only with our own loosely-developed brains, we must immediately figure out how to get those things within the first few seconds of life. Psychologists Harville Hendrix and Helen Hunt have made the point that these first few seconds, minutes, and days of our life will shape our entire experience of the world for a lifetime. Who is most likely to provide us with the things we need? How can we have those needs met? I am hungry; who will feed me? I am cold; who will swaddle me? If we do not get what we need, we will die. Yet, we have no experience in how to communicate those needs. We are born neuroscientists, trying to figure out how the human brain operates.
And yet. Here we are learning to be neuroscientists but at a much different level. How does the brain ensure an adequate blood supply for its needs? What part of the brain makes us recognize that a Dad Joke is funny, and prompts us to laugh (maybe a little) at it? What molecules change shape so that we can remember the smell of bread baking in our grandmother's kitchen, even 60 or 70 years after she has transitioned? More importantly in this moment, how can I alter the shape of my brain to pass this class?
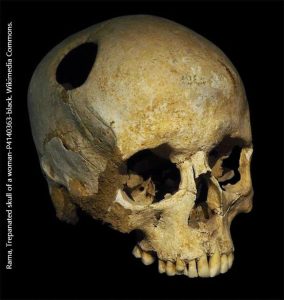
Knowing this, it should be no surprise that prehistoric cultures were struggling to figure out how human brains worked. Contrary to popular belief, they were not always wrong. In several different locations, at different times, humans figured out that if your brain begins to swell, your chances of survival were zero[1]. If an ancient shaman trepanned your skull, you were slightly more likely to survive. And so our ancestors did exactly that.

All across the globe, archaeologists have found human skulls with holes drilled or scraped in them. While humans used different technologies to create the holes in the skull, two incredible facts remain: they learned how to do it, and their patients sometimes survived. We know this because despite the surgical technique used, some (if not many) of the skulls show evidence of healing at the wound site.
 Although most of the skulls were found in European archeological digs, there was nothing special or unique about this method. In fact, one thing that argues for the "help someone recover from a head injury" vs the "cutting a hole to let out evil spirits" hypothesis is that the technique was invented independently in multiple locations. As we'd expect, the methods used were sometimes different in the Americas before the subjugation of indigenous people by European conquistadores.
Although most of the skulls were found in European archeological digs, there was nothing special or unique about this method. In fact, one thing that argues for the "help someone recover from a head injury" vs the "cutting a hole to let out evil spirits" hypothesis is that the technique was invented independently in multiple locations. As we'd expect, the methods used were sometimes different in the Americas before the subjugation of indigenous people by European conquistadores.
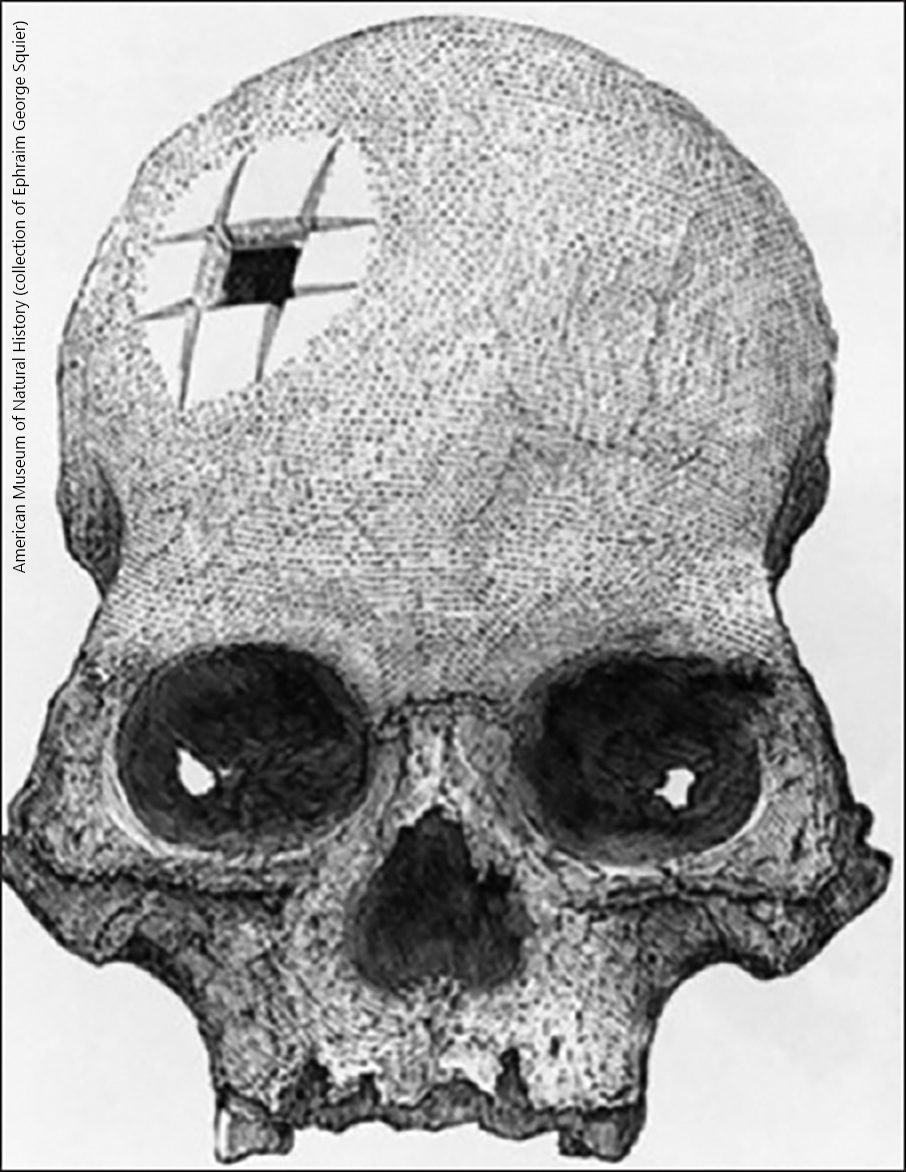
An example of the Eurocentric view of ancient trepanning is instructive. The skull shown here at left, with a set of incisions forming a square hole, was discovered at an Incan burial site and given to American archaeologist Ephraim George Squier. It shows clear evidence of wound healing. Yet the European surgeons of the mid-19th century refused to believe that Incan healers could master such a complicated surgical technique. It fell to the French neurosurgeon Paul Broca (who became famous for other reasons that we'll discuss a few pages later) demonstrated that there are several ways to gain access to the cranial vault using stone tools. He investigated at least four techniques to gain access to the brain, using different sorts of tools and proved that indigenous peoples were almost certainly capable of this skilled surgery.
Objective 3: Relate how the study of physiology, histology, and electricity led to a revolution in the understanding of neuroscience.
History of Neuroscience Objective 3 Video Lecture (coming soon)

At the beginning of the 19th century, neuroscience was a very tiny corner of biology. Any field of biology that existed in the 19th century, however, was greatly advanced by the observations of Charles Darwin as he voyaged on the HMS Beagle from 1831 to 1836. After becoming famous for his diary of the voyage, Darwin reorganized his observations on natural history as The Origin of Species, published in 1859. In it, Darwin proposed a theory of natural selection. There are two key elements to the theory. Traits are inherited from the parent, and vary amongst members of a species. Traits which increase fitness (i.e., the ability to reproduce) are more likely to be passed on to offspring; traits which decrease fitness are less likely to be passed on.
Behavior is a heritable trait, just like any other. This allows us to study the brain of different species to determine how those species are adapted to their individual ecological niches.
For example, dogs have an area in the frontal cortex called the prorean (or proreal) gyrus. Much of the herding behavior of the dog is due to activity of brain cells in the prorean gyrus. A dog's primordial ancestors had a rudimentary prorean gyrus which these species used to hunt in packs. Humans found this behavior useful for hunting, and over 30,000 years, selectively bred dogs for exceptional herding ability. At the end of this process, the prorean gyrus has become a much more elaborate and well-developed structure. This structural change parallels the incredible increase in herding ability in the modern domestic dog. The inheritance of a behavior (herding ability) is reflected in an anatomical change over evolutionary time.
As we select for behaviors in breeding experiments, we change the wiring and therefore the anatomy of the brain.
 Monkeys must find food by color and detail. The monkey visual cortex, in the back of the brain (toward the center of these photographs), is a highly organized and elaborate brain structure.
Monkeys must find food by color and detail. The monkey visual cortex, in the back of the brain (toward the center of these photographs), is a highly organized and elaborate brain structure.
 Rats crawl around in the dark. Rats don't need much visual cortex (in fact, in the lab, albino rats are essentially blind, yet they appear to behave pretty much like brown sighted rats). They do need detailed sensation from their vibrissae, the whiskers that protrude from their muzzle. In the brain cortex which senses touch, there are elaborate structures called barrel fields whose organization reflects this important function.
Rats crawl around in the dark. Rats don't need much visual cortex (in fact, in the lab, albino rats are essentially blind, yet they appear to behave pretty much like brown sighted rats). They do need detailed sensation from their vibrissae, the whiskers that protrude from their muzzle. In the brain cortex which senses touch, there are elaborate structures called barrel fields whose organization reflects this important function.

This photomicrograph of a flattened rat brain is stained for the mitochondrial enzyme cytochrome oxidase.

Each dark spot (barrel) represents exactly one vibrissae (hair on the muzzle).
Along with the advances in neuroscience driven by our understanding of natural selection, our advancement in an understanding of the electrical basis for nerve conduction came with another set of questions (as advances always do).
We know that electrical potentials spread in both directions along a wire. But is that true of electrical potentials traveling in the nervous system? The way in which nerve information travels as electrical potentials in the nervous system is governed by the Bell-Magendie Law.
About 1810, Charles Bell (working in Scotland) and François Magendie (working in France) more-or-less simultaneously approached the same question in the same way: are nerves unidirectional, sending information in one direction, or bidirectional like a wire, sending information in both directions?
 The spinal cord has dorsal (posterior) and ventral (anterior) roots, as shown in the diagram. (Dorsal means "toward the back" and ventral means "toward the belly"; the terms posterior "back" and anterior "front" replace these in human anatomy.)
The spinal cord has dorsal (posterior) and ventral (anterior) roots, as shown in the diagram. (Dorsal means "toward the back" and ventral means "toward the belly"; the terms posterior "back" and anterior "front" replace these in human anatomy.)
If Bell or Magendie cut the ventral (anterior) roots, paralysis resulted. The animal was unable to move a limb on the operated side.
If they cut the dorsal (posterior) roots, loss of sensation resulted.
Two important observations resulted from these experiments:
- the dorsal part of the spinal cord is responsible for managing sensory (feeling) information, while the the ventral part is responsible for generating motor (movement) information;
- individual nerve fibers carry information in only one direction under physiological conditions.
 Just as the dispute between Galvani and Volta dominated the late 18th century discussion of the electrical properties of the nervous system, and advanced the field in doing so, there was a less-polite scientific disagreement between Franz Joseph Gall and Marie Jean Pierre Flourens. Gall's ideas came to predominate 19th century neuroscience. He believed (correctly) that most brain functions were localized to specific areas of the human brain. He then concluded (incorrectly) that bumps on the skull were correlated with areas of larger and more complex development. Gall was responsible for the pseudoscience of phrenology, where a "practitioner" would feel the bumps on the skull and make representations about a person's abilities and interests.
Just as the dispute between Galvani and Volta dominated the late 18th century discussion of the electrical properties of the nervous system, and advanced the field in doing so, there was a less-polite scientific disagreement between Franz Joseph Gall and Marie Jean Pierre Flourens. Gall's ideas came to predominate 19th century neuroscience. He believed (correctly) that most brain functions were localized to specific areas of the human brain. He then concluded (incorrectly) that bumps on the skull were correlated with areas of larger and more complex development. Gall was responsible for the pseudoscience of phrenology, where a "practitioner" would feel the bumps on the skull and make representations about a person's abilities and interests.
Flourens, who believed (correctly) that the cerebellum is involved in the control of movement, criticized Gall on three grounds:
- ablation of the brain areas identified by Gall does not produce the results Gall would predict (correct);
- just because a bump exists on the skull, doesn't mean it has anything to do with the structure or size of the underlying brain part (correct);
- all areas of the cerebrum participate equally in sensory and motor functions (wrong).